“I do not consent my patients about the risk of pelvic floor injury for vaginal delivery. For the same reasons I don’t consent my patients about the risks of getting asthma from a c-section. The data is equivalently weak.”
These are the words spoken in April 2018 by Professor Neel Shah, the opening plenary session speaker at this week’s RCOG World Congress.
“These are long-term associations.
They are not causal and they are deeply confounded.”
[Watch from 38:56 to 39:26 here]
Furthermore, during the 2018 ACOG Irvin M. Cushner Memorial Lecture, “Cesarean Delivery Rate: Can it Be Safely Lowered”, Shah said:
“It is irresponsible to tell people they’re going to have pelvic floor injury from vaginal deliveries; it is equally irresponsible to tell them their baby is going to be obese, have asthma and other auto-immune diseases.“
Why does this matter?
This week it’s RCOG’s largest ever Congress; the event boasts attendance by 4,000 delegates from over 110 countries, in addition to social media coverage.
This is a tweet from Dr. Eddie Morris, soon to be the RCOG’s new President:

The RCOG tweeted:

And afterwards:

Dr. Morris tweeted:

In my view, withholding information from women about pelvic floor risk does not empower them, and neither is it safe nor supportive.
Other organisations highlight the need for informed consent too:

Renewed Focus on Caesarean Rates is Concerning
Professor Shah is a Director at the organisation Ariadne Labs, and works on its Delivery Decisions Initiative.
“His team is currently collaborating with hospitals across the United States, and using methods from design, systems engineering, and management to reduce the epidemic of avoidable c-sections.”
These are some #RCOG2019 retweets from Ariadne Labs:


Importantly, I did not hear Professor Shah’s RCOG talk, so my concerns are grounded in the talk I heard him give at ACOG last year, and why, 9 months after the UK’s CQC announced it would stop inspecting hospitals against caesarean target rates, the RCOG appears so enthusiastic about his views.
Coincidentally, ~200 miles north of the RCOG Congress, the Normal Labour and Birth 14th Research Conference began on the same day, with one of its presentations concluding with a call to “only use CS where medically required“, and “a call on health care providers, women agencies, women’s health advocates, and media to better communicate about CS” (see Twitter reaction thread here).
Those hosting #NormalBirth19, many of whom are proponents of reducing caesarean rates, support Professor Shah’s aims, and often include him in communication:


This is more understandable.
In October 2018, Professor Shah praised a Vox article by Julia Belluz (The troubling epidemic of unnecessary C-sections around the world, explained), which included the following recommendations:
How to stop the epidemic…

What women can do

In the same month, Dr. Eddie Morris tweeted:
Reading this description, I can’t help but be reminded of the NHS ‘Focus on Normal Birth and Reducing Caesarean section Rates Rapid Improvement Programme’, the NHS Institute for Innovation and Improvement’s ‘Toolkit for Reducing Caesarean Section Rates’, and the subsequent years of monitoring caesarean rates.
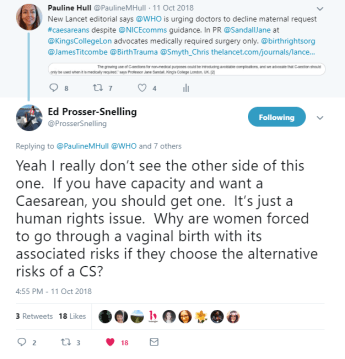
Again, based on Shah’s ACOG 2018 talk on caesarean rates, and examples like the article above, I was also concerned to read Dr. Ed Prosser-Snelling (one of the project team members with RCOG’s Each Baby Counts) suggesting that he provides
“a clear signpost of where we need to go“:

This is especially troubling given that my main criticism of the Each Baby Counts initiative is its exclusion of baby deaths prior to labour (and as such, advice to stay or go home that results in pre-labour foetal demise at full term is not counted)…
That said, Dr. Prosser-Snelling is a strong advocate for informed choice, including caesarean birth, so this made me wonder whether Professor Shah’s views on pelvic floor risk and consent are widely known.

RCOG Press Statement
To find out, I asked the RCOG’s press office:
1) Was/is the RCOG and/or Dr. Eddie Morris aware of Professor Shah’s views in relation to the communication of pelvic floor risks?
2) Does the RCOG agree or disagree with his view that the data on these two issues is equivalent?
3) Can the RCOG confirm whether it shares Professor Shah’s goal of ‘reducing caesarean rates’ going forward?
A spokesperson from the Royal College of Obstetricians and Gynaecologists (RCOG) provided me with the following statement today:
“The RCOG remains firmly committed to ensuring women’s voices and choices are always respected and supported to ensure the best possible birth and outcomes for a woman and her baby.
“As part of conversations between a woman and her healthcare professional, it is absolutely essential that women are fully informed of all the risks and benefits of all ways of giving birth, based on their individual circumstances and choices. This should include potential benefits and the small possible risks involved.**
“The RCOG continues to work with other healthcare organisations to ensure that information provided to women is impartial, accurate and evidence-based, to enable informed choice, safe and personalised care.”
This was very reassuring to read, but there are evidently still problems with how it works in practice.
Birth Wars?
For example, in a news report that aired on Australia’s The Feed in September 2018, the caesarean rate was debated again, and the programme asked:
“What’s safer, natural or caesarean?“
One of the mothers featured was Amy Dawes, a Brit living in Australia who last year helped found the Australian Birth Trauma Association following a pelvic floor injury.
She believes communication needs to be improved:
Another mother, Danielle, complains:
“I wasn’t educated on what could go wrong.”
The whole programme is worth watching, and although in this instance, debate between midwives and doctors is highlighted, the same issues arise in the UK too, and sometimes the strong disagreements that exist between doctors can be overlooked.
In fact:
– Many doctors disagree on the evidence.
– Many doctors disagree about what and how evidence is communicated.
Professor Shah’s opposite in the 2018 ACOG caesarean debate was Dr. Baha Sibai (based in the U.S.), and he argued that “Many of the recommendations and reasons used to encourage a reduction in C-sections are not justified or evidence-based.”
During their exchange he said, “The whole process of delaying second stage or using these forceps and vacuum produces something called stretch or avulsion of the levator ani muscle.
Now there are MRI studies being done, and very soon everyone’s going to wake up and say, ‘What have we been doing?‘”
[Watch from 42:45 to 43:14 here]
This undoubtedly makes antenatal communication challenging, and what I really want to highlight here is recognition of the difficulty maternity care faces moving forward, and the need to be honest and clear that divisions do exist.*
It’s not as simple as midwives versus obstetricians (in fact, that’s often not the case at all).
There can also be disagreement between midwives, and disagreement between doctors, and so I wonder, should this reality be acknowledged during antenatal discussions?
Knowing that there is more than one theory, and more than one pool of scientific data, might help women to understand and appraise the evidence, and to consider different birth plan options (both place and mode) alongside their own personal preferences.
With supportive systems then in place (thanks to the RCOG and the RCM working together), and NICE guidelines being followed, women would be at the centre of informed decision making (unless they prefer a more paternalistic approach).
I genuinely believe this could help to reduce subsequent anger about having preferences dismissed and information withheld:



Cost of Ignoring the Pelvic Floor
Last point.
The most obvious cost of discounting pelvic floor risk is the impact on women, both physically and mentally (see @BirthTrauma, @masic_uk, @MothersWith4DTs, @pelvicroar, @FibroidNetwork and others).
But there is also a significant financial cost.
A 2012 NHS report said “perineal trauma is one of the largest areas of litigation” in terms of claims concerning women, and this was 7 years ago (3 years prior to Montgomery).
Just one day before the RCOG Congress began, Caroline Zielinski, writing in Australia’s Illawara Mercury (‘They didn’t respect me as a mum’: Women sue doctors over birth trauma), explained:
“Korda is often called as an expert in birth trauma legal matters. He sees “one to two potential legal cases a week related to traumas associated with vaginal birth”, compared to three years ago, when he would only see “one to two cases a year”.
“In the wake of significant court cases here and overseas, law firms are reporting a steady increase in the number of women starting proceedings against hospitals and doctors over lack of information, following injuries sustained during vaginal births.
The same is evident in the UK, and Dr. Morris spoke only recently about the ‘big hidden cost’ of litigation:

And so, given the ever growing cost of maternity litigation, the law on consent and increasingly influential campaign groups, I would strongly suggest that the NHS can ill afford a maternity system design that advocates reducing caesarean rates at the expense of informed consent.
Additional Information
– For more information and conversation on this, follow #RCOG2019 on Twitter
*Extract from Lest We Forget – RCOG and others Enable and Encourage RCM’s Normal Birth Policies
**The RCOG confirmed subsequently that “small possible risks” here applies to all birth risks. The RCOG also provided this additional information:
– RCOG supports maternal request for caesareans, in line with NICE guidance. (2018)
– The World Health Organization (WHO) discourages the practice of aiming for target rates, and underscores the importance of focusing on the needs of women, on a case by case basis. (2015)
– The RCOG produces information for women, such as helping women to consider their birth options, for example, caesareans. (2015)
– RCOG and RCM endorsed two NHS guides to help explain birth choices for women:
Your choice: where to have your baby – for women having their first baby
Your choice: where to have your baby – for women who have had a baby before
– Some of the information here was included in my October 2018 Grand Rounds presentation at the University of Calgary’s Department of Obstetrics & Gynecology.
- Written by author and journalist Pauline Hull
With thanks to the RCOG press office for its timely response during such a busy event.

I suffered avulsion as a result of a vaginal delivery and forceps. This is very common but no one talks about it! Shocking to see how careless comments are made by (male) doctors on this – they don’t have to live with the consequences!
LikeLike
Denying the damage done as a direct consequence of vaginal delivery is tantamount to the nonsense spread by anti-vaxers.
Women have a right to full facts of potential damage to them as a result of vaginal birth just as much as they do when planning a Caesarean section. It is for women to decide what risks they are willing to take in relation to their own bodies. The days of ‘doctor knows best’ are gone (Montgomery v Lanarkshire).
LikeLike
Pelvic floor risks should absolutely be discussed in the prenatal period. I am an RN, read multiple prenatal books, took prenatal classes, and had a high risk pregnancy related to advanced maternal age, gestational diabetes, large baby, and history of failure to progress resulting in emergency cesarean. Not one single health care professional mentioned pelvic floor risks such as prolapse. Nobody told me to take it easy postpartum. My husband was back at work less than 72 hours after my delivery, so I was left home alone with a newborn and no family or friends nearby. There was no resting or recovering for me postpartum, I didn’t even know I should be taking it easy. Well, I ended up with grade 3-4 rectocele and cystourethrocele and 1.5 uterine prolapse, plus rectal prolapse (which only affects 3 in 100,000). Because I way overdid it early postpartum, between being active and lifting and getting constipated. Because not one single healthcare professional mentioned any risks to me. I now have zero quality of life and am suicidal because I cannot imagine living another 50 years with organs falling out of my body, fecal incontinence, and constant rectal pain and pressure. I would give anything and everything to go back and either elect for repeat cesarean or at least take it easy for a few weeks after birth (I prolapsed at 2 weeks pp after majorly overdoing it for 10 days). I feel so let down and betrayed by the medical community, I feel powerless and helpless and devastated and so angry that so many health care professionals could have helped prevent this or lessen the severity and remove some of the distress and shock and devastation of prolapse, if it had just been mentioned even once. One of my prenatal books had a section on vasectomy but not a word about prolapse. What kind of disservice is this to women?! I can guarantee you if men’s organs were falling out of their penises, the medical community would be warning and educating about it, and investing a lot more money in prevention and treatment. I have not been able to enjoy a single day since my daughter was born 9 months ago. I feel robbed of my life. And she may someday be robbed of a mother because I don’t think I can live this life of pain and frustration much longer. So so disappointed in the medical community. Come out of the dark ages and start supporting women better. Seriously. We deserve better.
LikeLiked by 1 person
I’m so sorry to read this Erin, and you’re right, women deserve better. I hope you have been able to access support, whether that’s through the NHS or perhaps an organisation like the Birth Trauma Association. There are also some support groups online for women with pelvic floor injuries, many of whom feel similarly devastated when this happens to them. It’s important that you are helped to see a way forward in all this. Again, I’m very sorry, and thank you for being brave enough to share your experience here.
LikeLike
Another one damaged by vaginal birth…pelvic floor damage is very real. It is not disclosed in my experience from your midwife.
All this damage and the pressure of the baby coming down causes prolapse, discomfort and pain. No one tells you this beforehand and after it seems that no one cares.
One day the truth will out and the tide of maternal request caesereans will be unstoppable. At the very least risky forceps deliveries won’t be tolerated and practices around induction etc will change. Once all risks are disclosed…all forms of birth will improve as women will know and pressure health professionals to help them emerge relatively unscathed!
LikeLike