Today’s 2018 survey of women’s experiences of maternity care, published by the Care Quality Commission, is symptomatic of a serious problem within NHS maternity care, communication, policy and guidance.
Caesarean birth is too often ignored and/or marginalised.
For example, the CQC’s NHS Patient Survey Programme explains how:
“NICE clinical guidance states that pregnant women should be offered evidence based information and support to enable them to make informed decisions about childbirth.” (p.21)
However, while the document cites 11 NICE guidelines, quality standards and documents >30 times in total, recommendations on caesarean birth are entirely absent.
Excluded:
CG132 Caesarean section
QS32 Caesarean section
Included:
CG62 Antenatal care for uncomplicated pregnancies
QS22 Antenatal care
CG190 Intrapartum care for healthy women and babies
QS105 Intrapartum care
QS115 Antenatal and postnatal mental health
QS37 Postnatal care
CG37 Postnatal care up to 8 weeks after birth
QS15 Patient experience in adult NHS services
QS129 Contraception
NICE Impact Maternity (May 2018)
Pregnancy and complex social factors: a model for service provision for pregnant women with complex social factors (September 2010)
Caesarean birth is referred to just four times, and only as something to be avoided or reduced:
- “Care during labour and birth… Some studies have shown that being admitted to hospital too early on in labour can cause certain complications, such as increased risk of caesarean section, and health professionals recommend that women stay at home until contractions become frequent. Therefore, it is important to provide advice and reassurance to women in early labour about how long they can stay at home. Eighty-six per cent of respondents said that at the very start of their labour, they felt they were given appropriate advice and support when contacting a midwife or the hospital, leaving 14% who felt they did not.” (p.25)
When advice to stay home is based on trying to reduce the likelihood of a caesarean birth, if loss or injury occurs, 14% becomes a big number when litigation costs are factored in.
- “Involvement and support… Thinking about your care during labour and birth, were you involved enough in decisions about your care? All current national policy and guidance state that one-to-one midwifery care should be provided to women in established labour. A Cochrane review looking at continuous support during labour suggests that this can improve outcomes for both mother and baby, for example, shorter duration of labour, and decreased caesarean birth, decreased instrumental vaginal birth.” (p.31)
NICE guidance has stated since 2011 that obstetrician care and support for their choice should be provided to women who request a caesarean, but this is not cited.
- “Northern Ireland… Areas for concern include that caesarean section rates remain high with just over half of these planned.” (p.56)
This is particularly disappointing given the CQC’s assurances in September 2018 that “going forward the wording used in our reports is clear and reflects our position in ensuring safe maternity care rather than appearing to encourage one approach over another.”
While this a statistical release (not an inspection report), and the actual data was collected before September, the CQC’s summary wording here has been published at the end of January 2019.
- There is also this table. (p.28)
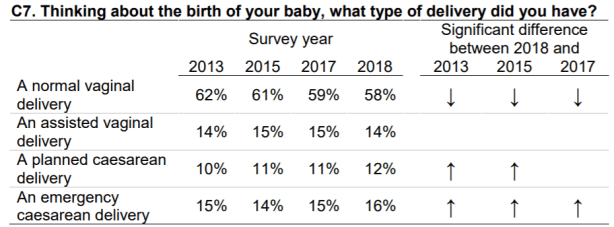
Many women consider their caesarean births ‘normal’ too, but that debate aside, what is the purpose of this table? What do the arrows up and down signify? Why is this difference such a key focus? I ask this in the context of the CQC’s comments on Northern Ireland’s caesarean rates above.
CQC is not alone
The CQC cites the NICEimpact maternity document in its maternity survey, and while I am critical of the CQC’s exclusion of caesarean birth guidelines and standards, it’s perhaps more shocking to discover that the National Institute for Health and Care Excellence itself did the exact same in May 2018:
- “Choice of birth settings and antenatal services
The Maternity Transformation Programme aims to widen and deepen choices available for women. NICE recommends that women should have the choice of different birth settings; more alongside midwifery units are now available and women are increasingly being offered this option. NICE’s guideline on intrapartum care for healthy women and babies sets out the evidence for the safety of different birth settings and recommends that women should be given the choice of where to give birth. The guideline lists 4 birth settings which should be offered to women who are at low risk of complications: home, freestanding midwifery unit, alongside midwifery unit and obstetric unit…“The CQC maternity survey collected the experiences of over 18,000 women who gave birth in 2017. The survey asked whether they were given the option of different birth settings… the proportion of women who said they were offered a choice of giving birth in a midwife-led unit or birth centre has increased to 42%, up from 35% in 2013. The NMPA organisational survey also looked at choice in antenatal services…” (p.14-15)
NICE makes no reference to CG132 or QS32 on caesarean birth, and does not cite its own recommendations regarding choice of different birth modes.
- “Decision-making and experiences of care
All of NICE’s maternity guidance is underpinned by the principle that women should be treated with respect and dignity, and involved in decisions about their own care. The CQC maternity survey records how well women feel these principles were achieved. In order to make choices and decisions about their care, women need access to good quality information. NICE’s guideline on antenatal care recommends that, at each antenatal appointment, healthcare professionals should offer consistent information and clear explanations, and should provide pregnant women with an opportunity to discuss issues and ask questions.” (p.16)
The statements in bold above should include information on caesarean birth.
- “What happens next?
This report highlights some positive progress in the uptake of NICE recommendations for safe and personalised maternity care…
Many of the interventions supported by the Maternity Transformation Programme, on safety, prevention, workforce, women’s choice and the personalisation of care, are underpinned by NICE recommendations.” (p.18)
Again, positive progress, choice and personalisation of care is confined to improving information and choice around vaginal birth.
Women are increasingly seeing through this smoke screen, and it’s evident to many that unless it achieves greater balance, the NHS cannot and will not stem the tide of maternity litigation.
When choice is not a choice
Lastly, in its sections headed ‘Choice‘, the CQC survey confidently assures readers that:
- “All recent national maternity policy has promoted women’s choice of place of birth.
Women’s choice and personalised care is also one of the priorities of the Maternity Transformation Programme.” (p.19)”Better Births highlights the need for clear unbiased information to help women make decisions around labour and birth, such as around pain relief.” (p.26)
This is simply not true for caesarean birth choice, at least currently.
Back in February 2016, I wrote about my disappointment with the Better Births National Maternity Review, and my concern that it had ignored planned caesarean birth benefits and choice.
So far, this has come to fruition.
Hope for the future
To close on a more positive note however…
In October 2018, Caesarean Birth was given the opportunity to give feedback during the CQC’s 2019 maternity survey stakeholder consultation process, and I am very hopeful that caesarean birth will be better represented in its next annual release.
It’s also important to recognise that the CQC is not alone in omitting caesarean birth information in this way, and I hope this summary shines a light on how much work there is still to do – more than 7 years post CG132 recommendations – to give mode of birth an equal footing with place of birth when it comes to informed choice.
- Written author and journalist by Pauline Hull
(Both NICE and the CQC have been contacted for further information.)
