Milton Keynes University Hospital NHS Foundation Trust (MKUH) policy:
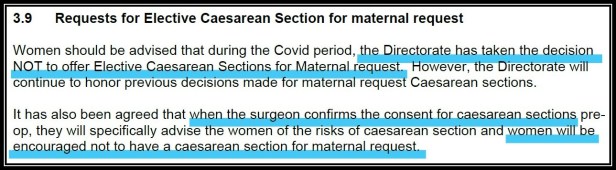 Pandemic or no pandemic, the extract above makes a mockery of the 2015 Montgomery v Lanarkshire Health Board Supreme Court judgment on informed consent and the 2011 NICE CG132 recommendations on maternal request caesarean birth.
Pandemic or no pandemic, the extract above makes a mockery of the 2015 Montgomery v Lanarkshire Health Board Supreme Court judgment on informed consent and the 2011 NICE CG132 recommendations on maternal request caesarean birth.
Under cover of COVID-19, and with a review date of April 2021, MKUH has published this policy in its new Standard Operating Procedure, despite no new evidence of increased risk or cost with planned caesarean birth versus planned vaginal birth.
And despite its own ‘Maternity Services‘ promise…
May 5th 2020
A woman in her third trimester of pregnancy contacted Caesarean Birth to say her prophylactic caesarean birth plan had been refused by a consultant at MKUH during a phone conversation, and without any discussion of the reasons for this choice. The woman said she was told to contact her GP if she wanted to pursue it any further.
Twitter exchange with @MKHospital…

May 6th 2020
Since the woman’s experience and the hospital’s reassurance via Twitter did not align, I sought further clarification from MKUH, and also emailed its communications team to request formal confirmation of its planned caesarean birth policy (no response to date*).
Tweet to @MKHospital (no further response)…

May 7th 2020
I received a copy of MKUH’s SOP and clinical pathway for Consultant Antenatal Clinics, ADAU, Growth scans during evolving Covid-19 pandemic, which confirmed a “decision
NOT to offer Elective Caesarean Sections for Maternal request“.
This was not surprising, since I was already aware from other communication with women during COVID-19 that some hospitals are not supporting prophylactic caesarean birth plans, but I was shocked to learn that at the eleventh hour, during their pre-op consent, women who have had this birth plan agreed previously will be “encouraged not to have a caesarean“.
Important note:
This is 5 years post-Montgomery; currently 70% of the £78 billion Clinical Negligence Scheme for Trusts relates to maternity (in 2018/19 the cost of harm was ~£9 billion, of which ~60% related to maternity claims); and a 2019 litigation analysis concluded “there is no justification to deny or discourage planned Caesarean section on grounds of cost“.

Also worth noting is the number of medical professional Stakeholders who are listed as having consulted and approved the publication of this policy (7 midwives; 2 OBGYN consultants; 2 OBGYN registrars; fetal medicine consultant; labour ward manager; matron; superintendent sonographer; chair of the Trust Documentation Committee; and Medical Director chair of the Clinical Board).
Also: “This SOP has been written in response to the current global Covid 19 pandemic and follows the directive from Associate Director of Operations, Women’s and Children’s Health and supported by the Clinical Services Lead (CSL) for Obstetrics and Gynaecology.”
This is concerning because it suggests the prophylactic nature of ‘maternal request’ caesarean birth may still not be fully understood. It is not simply a ‘choice’ or ‘preference’ for most of the women (and medical professionals) who request it. It is an informed decision based on careful consideration of the risks and benefits of each planned birth mode, and choosing to reduce the risks associated with instrumental delivery and/or emergency surgery (for example) is evidently justified.
May 9th 2020
This would have been the 12th birthday of Ebony McCall, who died 14 minutes after she was born at Milton Keynes General Hospital in 2008.
A PA/Independent report by Ellen Branagh on the inquest into Ebony’s death explained how her 17 year-old mother Amanda, who “suffered medical conditions, including cardiac disease“, was denied an elective caesarean birth plan.
Instead, induction was advised; she “refused because of the pain and requested a Caesarean section but was told these could only be given at night if they were emergencies.” When labour began naturally that night, “the baby’s heartbeat became erratic, necessitating the emergency Caesarean she had wanted in the first place.”
Frustratingly, situations like this are still happening in 2020.
May 11th 2020
I read this BMJ interview with MKUH Medical Director Dr. Ian Reckless, in which he explains, “In Milton Keynes, we were early off the starting blocks with respect to COVID-19. We hosted one of the two repatriation and quarantine centres for residents of Wuhan Province returning to the UK in February. This got us thinking about infection prevention and control, and novel clinical pathways some weeks ahead of our peers.”
I don’t believe Dr. Reckless was necessarily speaking in the context of maternity care pathways, but I include it here because it highlights how other NHS hospitals (peers) could decide to follow the MKUH’s lead for women who want to plan a caesarean birth, if they haven’t already done so.
May 12th 2020
With permission from the woman who contacted me, I have written to the CEO and Medical Director of MKUH to request that the Trust reconsider this policy, both in her individual case and for any other women who might want to plan a caesarean birth during the pandemic.
More to come…

Even before COVID-19, at least 15% of Trusts had policies or processes that did not explicitly support maternal request caesarean birth (Birthrights, 2018), and this inconsistency and confusion is likely even more pronounced for women during the pandemic; in part due to the communication and information from organisations including the Royal College of Obstetricians and Gynaecologists, the Royal College of Midwives and NHS England.
There is no new evidence to suggest that (compared with planning a vaginal birth) planning a caesarean birth is of greater risk for women, their babies or maternity care staff than it was pre-pandemic. As such, and especially post-Montgomery, NICE recommendations should still be followed.
Lastly, given that more women choose to plan a caesarean birth than a home birth, it may be fair to question (both now and in the future) whether the attention and support afforded the two choices throughout COVID-19 has been proportionate or fair.
This picture was sent to me in 2013…

A woman told me she was brought into a room to discuss her caesarean birth request only to see this on the wall above her head. I often wonder, what will it take for the NHS to put an end to all this?
- Written by author and journalist Pauline M Hull
*A member of the communications team has now responded to apologise for the delay and explain that this is an extremely busy time. This is completely understandable, and I will update this article with any further communication or statement in due course.

I am living in Milton Keynes , and for sure I will not be willing to have my birth plan on Milton Keynes hospital. Is unacceptable to use this pandemic as an excuse for not allowing a women to exercise her right to chose her birth plan.
LikeLike
Completely unacceptable. There has been no evidence-based guidance that c sections should be limited due to COVID-19. Safe, personalised maternity care is not an optional extra. Particularly awful too that the policy is to try and derail birth plans at the point where the woman has come to hospital to have her baby – that must be very upsetting to go through. Looks like an excuse to deny maternal request c section.
LikeLike
Having come out of a horrifying Kiellands forceps delivery with no choice offered to proceed straight to c section…I am disturbed that the Corona virus pandemic seems to be being used to force vaginal birth at all cost. Birth when it goes wrong is life affecting and women need to feel cared for and their birth choices respected.
I don’t believe I will have another child now due to the trauma, so the benefits for forceps when baby was high (not low as I was told) have diminished. As the only reason for avoiding a c section in that situation is for future pregnancies …
Women who don’t want to deliver vaginally should have the option of a c section according to Nice guidelines. I really feel for any pregnant women now caught up in the pandemic who are not only stressed about Corona virus, but are also wondering if they will be able to have the birth they want and more importantly need.
LikeLike
I requested a c section with my first child at MKHospital in 2016 as I had been diagnosed with M.E and was concerned as to how my energy levels would be if I had a long labour as many in my family had before me. I was refused a c section and told by the consultant ‘I was about to become a mother I needed to find some courage’. Absolutely disgraceful!
LikeLike